
Erythema Multiforme: What do we know?
By Dr. Chanran Ganta
What is Erythema Multiforme?
|
|
Erythema Multiforme (EM) is a cutaneous reaction pattern of multifactorial etiology that is seen in dogs, cats, horses, cows and ferrets. The pathophysiology of EM is thought to be a host-specific T-cell mediated hypersensitivity. The cellular immune response is directed against various keratinocyte-associated antigens, including those associated with drugs, infections (viral, fungal, bacterial), neoplasia, various chemicals, foods and connective tissue diseases. CD8+ T lymphocytes bind to antigenically altered keratinocytes and trigger apoptosis of keratinocytes/squamous epithelial cells. Based on the extent of involvement throughout the body, it is classified as erythema minor, erythema major, Stevens-Johnson syndrome or toxic epidermal necrolysis.
What is the trigger?
The highest frequency of cases reported in dogs, cats and horses with EM are drug-induced. The drugs that are commonly associated with EM include trimethoprim potentiated sulfonamides, penicillins and cephalosporins. Other causes of EM that are less frequently reported include dyes and preservatives in food, vaccination with Bordetella bronchiseptica, parvoviral infection, and insecticidal dips.
What are the clinical signs?
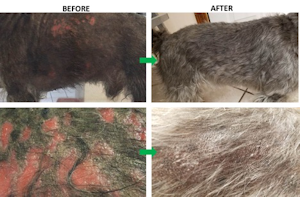
There will be an acute onset of erythematous annular macules, elevated circular plaques and papules that can be partially symmetric. In some cases, these lesions appear as classic targetoid with concentric circular zones of erythema, blanching and exfoliation. These lesions most commonly occur on the trunk and especially involve the glabrous skin of the groin and axilla. Other common sites of involvement include mucocutaneous junctions, oral mucosa, pinna and pawpads (Figures 1-2). German Shepherd dogs and Pembroke Welsh Corgis were reported to be at increased risk. There is no breed predilection in other species.
How do you diagnose ?
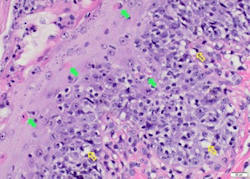
The differential diagnoses for this condition includes urticarial allergic eruption, superficial spreading pyoderma, bacterial folliculitis, dermatophytosis, demodicosis and early lesions of bullous autoimmune diseases. A definitive diagnosis can be reached by histopathology. It is important to acquire a good biopsy for a definitive diagnosis of this condition. The biopsy needs to be collected from areas of erythema without crusting or ulceration with INTACT epidermis or mucosa. Characteristic histopathological lesions include apoptotic epidermal cells/keratinocytes at all levels of the epidermis, vacuolation of the basement membrane zone, few lymphocytes surrounding apoptotic keratinocytes and interface dermatitis (Microscopic Image 400X; Solid arrows: Apoptotic keratinocytes; Open arrow: Basal cell vacuolation).
Please contact Dr. Ganta or Dr. Bagladi if you have any questions regards sample collection and any skin diseases related questions.