
May 2018
Canine Solar Dermatitis
|
||
|
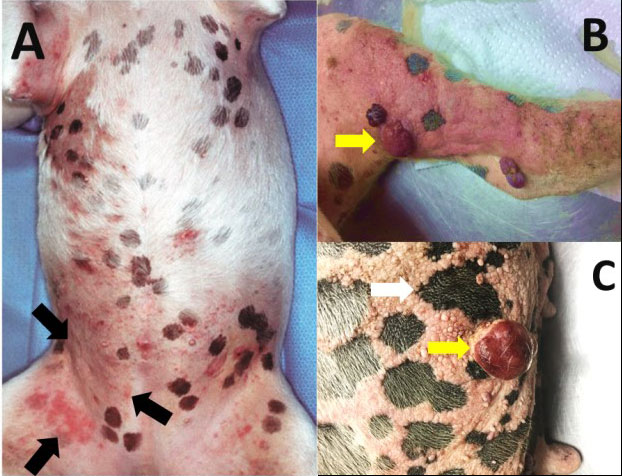
Figure 1: Dermal lesions noticed mostly on the ventrum nclude erythema, crusting (black arrows) and nodules identified as hemagiosarcoma (yellow arrows). A sharp demarcation in epidermal changes noticed in pigmented and nonpigmented areas (white arrow). Image courtesy: Dr. Ann Hargis, De Soto (Kansas) Veterinary Clinic. |
||
|
||
|
||
| Figure 3: Perivascular cuffing is present with gitter cells (macrophages), lymphocytes, and plasma cells (arrows). Congestion of the vessel (V) is present with mild perivascular hemorrhage. |
By Drs. Charan Ganta and Sarah Schneider
What is solar dermatitis?
Canine solar dermatitis or chronic sun burn is a severe dermatologic disorder that often occurs on the medial aspect of the legs, ventrolateral abdomen and thorax, lateral flank, and bridge of nose in non-pigmented skin. The distribution of the lesion is dependent on the individual animal behavior and length of exposure. The lesions usually start as erythema and scaling which will evolve into thick, firm and wrinkled skin, with alopecia, comedones (dilated hair follicles) with occasional round raised red nodular masses (Figure 1). The haircoat, stratum corneum, and melanin pigmentation usually protect against the harmful effects of UV radiation. However certain breeds with short hair coat and or light pigmention like Beagles, Boxers, Bull Terriers, Dalmatians, Pit bulls, Whippets etc. are more frequently affected. Figure 1B & C shows a 5-year-old boxer with black spots demonstrating sharp demarcation between areas of normal skin with dark pigment and damaged unpigmented skin showing marked epidermal hyperplasia and erythema, suggestive of the protective effects of melanin pigmentation.
Pathogenesis
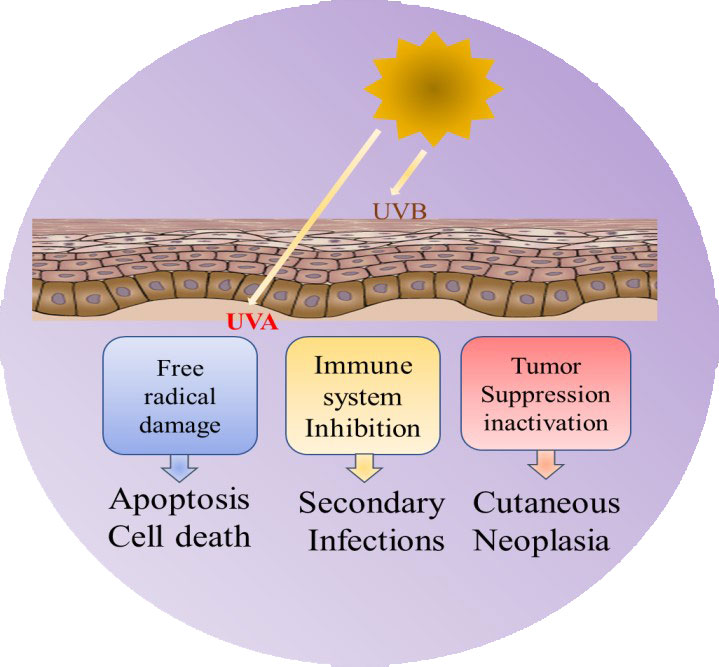
Long term direct exposure to high energy ultraviolet radiation, UVA (320-400 nm) and UVB range (290-320 nm) leads to phototoxicity. The three important cellular events include 1. Oxidative damage and cell death; 2. Immune suppression; 3. Inhibition of tumor suppression. High energy UV radiation causes direct damage to keratinocytes via free radical damage and release of proinflammatory cytokines that enhance tissue injury and cell death along with weakened immune system leading to secondary infections. Intermittent chronic exposure causes keratinocyte proliferation, mutagenesis, and premalignant actinic keratosis which can evolve into sun-induced skin tumors like squamous cell carcinoma, hemangioma, and cutaneous hemangiosarcoma.
Clinical Diagnosis
The skin lesion initially manifests as erythema and scaling which often resemble pyoderma, dermatophyte infection, cutaneous lymphoma or an autoimmune disease. Hence an adequate history (including history of sun bathing/sun exposure), patient signalment, duration, distribution and location of the lesions and non-responsiveness to standard of care therapy are often helpful in ruling out solar dermatitis.
Biopsy Collection and Histopathology
A definitive diagnosis can only be reached by histopathological examination of the skin biopsy. We recommend collection of multiple skin biopsies at different stages of the disease. Based on the presentation of the gross lesions, often the samples should include areas of erythema, crusted plaques, nodules, and margins of ulcers to see the full spectrum of the disease. Solitary nodules should be completely excised to prevent overt progression of neoplasia. In the event of secondary pyoderma, biopsies should be collected post antibiotic therapy to prevent misdiagnosis.
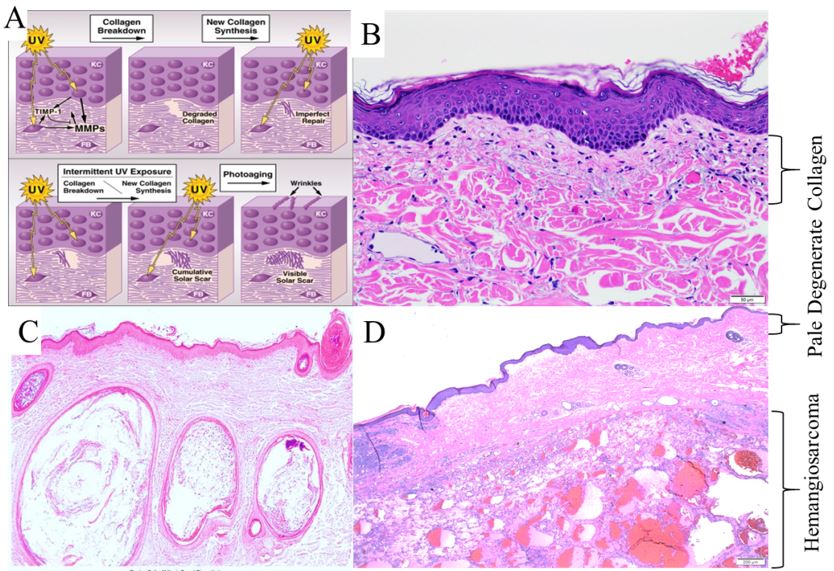
The most consistent histologic finding in dogs with chronic solar dermatitis is a narrow, hypocellular, pale-staining band of collagen along the dermo-epidermal junction with deposition of numerous pale blue stained elastin fibers (Figure 2B). Epidermal hyperplasia, follicular dilation with keratosis (comedones) and dermal fibrosis is often noticed. In chronically exposed severe cases, concurrent UV light–induced neoplasms, such as hemangioma, hemangio-sarcoma (Figure 2D), or squamous cell carcinoma could be noticed.
Treatment
The best treatment option is to minimize the exposure to sunlight. Additional treatment options are available. Due to the scope of this newsletter, they are not listed here, we recommend contacting the KSU-CVM Veterinary Health Center at 785-532-5690 for treatment and management options.
Questions or comments: ckganta@vet.k-state.edu
References
(Provided on request)
For more information contact KSVDL Client Care at 866-512-5650 or clientcare@vet.k-state.edu.