
September 2017
West Nile Virus in Kansas
By Drs. Mike Moore and Katie Delph
History
Since its introduction into North America in 1999, West Nile Virus (WNV) has spread and is now endemic across the US and parts of Canada and Mexico.
In August 2017, the Kansas State Veterinary Diagnostic Laboratory (KSVDL) confirmed a case of WNV in a horse from Kansas. This adds Kansas to a list of 12 other states confirming 39 recent cases of WNV in horses. This list includes the neighboring states of Colorado and Missouri.
Clinical signs
WNV clinical signs in the horse are highly variable and can include mild fever, feed refusal, and depression without neurologic signs. The neurologic signs that may be present are highly variable, but spinal cord disease and moderate mental aberrations are the most consistent. Spinal cord disease manifests as asymmetric, multifocal or diffuse ataxia and paresis.¹ Less common clinical signs include cranial nerve deficits such as facial nerve paralysis. These signs are difficult to differentiate, without diagnostic tests, from other viral encephalopathies that may be encountered by practitioners, including EEE, WEE, and rabies.
Transmission and Prevalence
WNV is endemic in many reservoir perching-bird populations. Mosquitoes are the vector that transmit the WNV virus from birds to horses and people. Clinical cases in horses tend to cluster in the late summer and fall after increased mosquito activity.
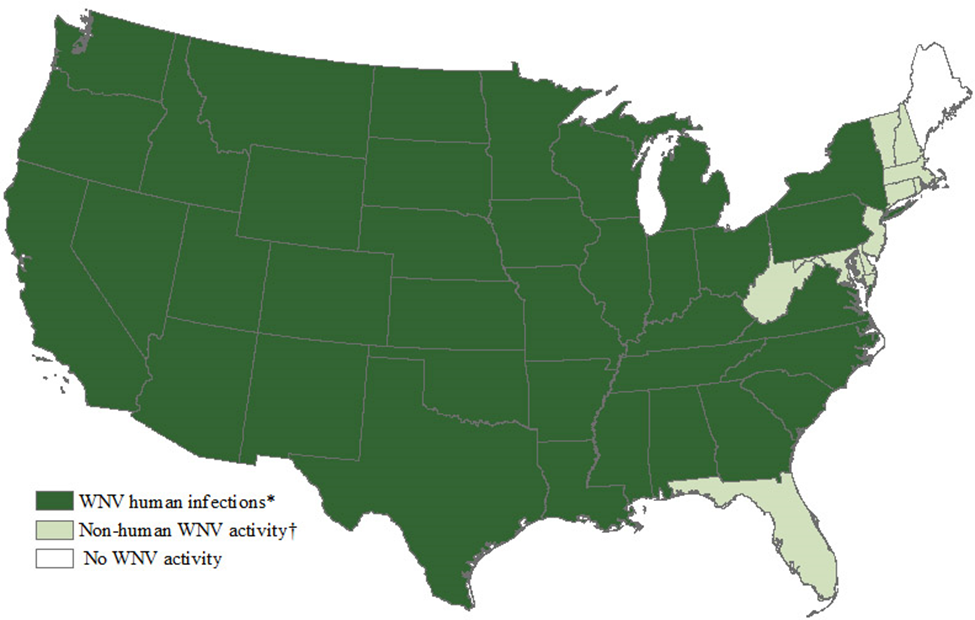
The Centers for Disease Control and Prevention (CDC) reports as of September 5, a total of 47 states and the District of Columbia have reported West Nile virus infections in people, birds, or mosquitoes in 2017 (Figure 1) Overall, 526 cases of West Nile virus disease in people have been reported to the CDC. Of these, 303 (58%) were classified as neuroinvasive disease (such as meningitis or encephalitis) and 223 (42%) were classified as non-neuroinvasive disease.²
Diagnostics
Ante mortem diagnosis can be accomplished with an IgM ELISA test. This test can be completed on 0.5 ml of serum or cerebral spinal fluid. For neurologic cases, high levels of IgM in the serum, along with clinical signs, can provide a presumptive diagnosis. Elevated IgM in the CSF is definitive.
Post mortem diagnosis is best accomplished by PCR. A one gram sample of brain is required and the estimated turnaround time is two days.
For more information on WNV testing, contact KSVDL at clientcare@vet.k-state.edu or 866-512-5650.
References
¹ Long, Maureen. “Overview of Equine Arboviral Encephalomyelitis”
http://www.merckvetmanual.com/nervous-system/equine-arboviral-encephalomyelitis/overview-of-equine-arboviral-encephalomyelitis#v21432862
² CDC “West Nile Virus Activity by State – United States, 2017 (as of September 5, 2017)”
https://www.cdc.gov/westnile/statsmaps/preliminarymapsdata2017/activitystate.html
Dr. Jamie Henningson appointed interim KSVDL Director
Return to Index